If you've been researching CIRS, you've almost certainly come across the term MARCoNS. It comes up in treatment forums, in conversation about why some people don't improve even after leaving a moldy building, and in the protocols of physicians who specialize in biotoxin illness. It's also a term that raises real questions, because mainstream medicine hasn't fully adopted it, the research base is narrow, and the explanations you find online range from careful to wildly overstated.
This is an attempt at a clear, honest explanation of what MARCoNS actually is, where it fits within the CIRS framework, and what remains genuinely uncertain.
What MARCoNS means and where the term comes from
MARCoNS stands for Multiple Antibiotic Resistant Coagulase Negative Staphylococci. It refers to antibiotic-resistant strains of coagulase-negative staphylococcal bacteria found in the nasal passages, specifically embedded in a biofilm. A biofilm is a protective matrix that communities of microorganisms produce around themselves. Within a biofilm, bacteria are significantly more resistant to antibiotics and to the body's normal immune responses than they would be in free-floating form.
Coagulase-negative staphylococci are common bacteria. They exist on skin and in nasal passages in the general population and are not inherently pathological. The concern in the MARCoNS context is specific: multi-drug resistant strains, living in a biofilm in the deep nasal passages, in individuals who are already immunologically compromised by biotoxin exposure.
The term was developed and introduced within the CIRS research framework by Dr. Ritchie Shoemaker, who proposed that MARCoNS colonization in CIRS patients contributes to ongoing immune dysregulation and prevents recovery even when the individual has left the contaminated environment. In the Shoemaker protocol, testing for and treating MARCoNS is a formal step in CIRS management.
How MARCoNS is thought to perpetuate CIRS
The proposed mechanism is worth understanding, along with its limitations.
According to the Shoemaker framework, the bacteria in a MARCoNS biofilm produce hemolysins, enzymes that can degrade proteins, including alpha-MSH, a peptide that plays an important role in regulating inflammation and immune signaling. Alpha-MSH suppression is documented in a subset of CIRS patients and is associated with ongoing inflammatory dysregulation, impaired mucosal immunity, and difficulty with biotoxin clearance.
The hypothesis, then, is a cycle: biotoxin exposure from a water-damaged building creates immune suppression and reduced alpha-MSH; this creates conditions in the nasal passages that favor MARCoNS colonization; MARCoNS biofilm produces hemolysins that further suppress alpha-MSH; and this perpetuates the inflammatory state even after the external exposure source has been removed.
This is a biologically plausible hypothesis. It is grounded in known mechanisms of biofilm persistence and the documented role of alpha-MSH in immune regulation. But it is important to be precise about the evidence base. The research supporting this specific chain of causation in CIRS patients is limited largely to clinical observations, case series, and work published by or affiliated with researchers within the Shoemaker network. It has not been independently replicated in large, controlled trials. Mainstream infectious disease and otolaryngology do not recognize MARCoNS as a distinct clinical entity, and there is no independent consensus on its prevalence, its causal role in CIRS, or the appropriate standard of care for treating it.
That doesn't make the framework wrong. It means the science is still developing, and claims should be proportionate to what the evidence actually demonstrates.
How MARCoNS is identified
Testing for MARCoNS involves a deep nasal swab, sampling from the area near the back of the nasal passages rather than a standard superficial swab. The sample is cultured and tested for antibiotic sensitivity to determine whether resistant coagulase-negative staphylococci are present.
This testing is not a standard part of conventional medical practice. It is typically ordered by physicians who use the Shoemaker protocol or who practice functional or integrative medicine with an orientation toward mold illness and biotoxin conditions. A positive result means antibiotic-resistant coagulase-negative staph was found in the nasal biofilm. It does not, on its own, tell you whether that colonization is causing harm, whether it is a consequence of CIRS or an independent finding, or whether treatment will change your clinical trajectory. Those questions require clinical judgment by a physician familiar with the full picture.
What treatment typically looks like, and what to know about it
Treatment in the Shoemaker protocol has typically involved a compounded nasal spray, most commonly containing BEG, a combination of bismuth, EDTA, and gentamicin. The goal is to disrupt the biofilm and reduce the bacterial load in the nasal passages.
Gentamicin is an antibiotic that, when used systemically, carries known risks including nephrotoxicity and ototoxicity. In a compounded nasal spray at low concentrations, the systemic absorption is limited, but this is still a consideration that should be discussed with a prescribing physician. Not every compounding pharmacy produces these preparations with identical concentrations or quality controls, and there are no large randomized controlled trials establishing the safety and efficacy of BEG spray specifically in CIRS patients.
Some clinicians now use alternative agents. As with much of the CIRS treatment space, the evidence base for specific protocols is limited by the absence of large, independently conducted trials. This is not a reason to dismiss patient experiences, many of whom report meaningful improvement following MARCoNS treatment. It is a reason to approach any treatment decision in this area in close partnership with a qualified physician, not based on online recommendations alone.
What this means for your home environment
If MARCoNS is a factor in your ongoing CIRS, it underscores something that comes up consistently in the clinical literature: sustained recovery from CIRS requires removing ongoing environmental triggers. A nasal biofilm doesn't form in a vacuum. Conditions that created immune suppression and mucosal vulnerability in the first place, primarily continued exposure to water-damaged building environments, are also conditions that make recolonization more likely.
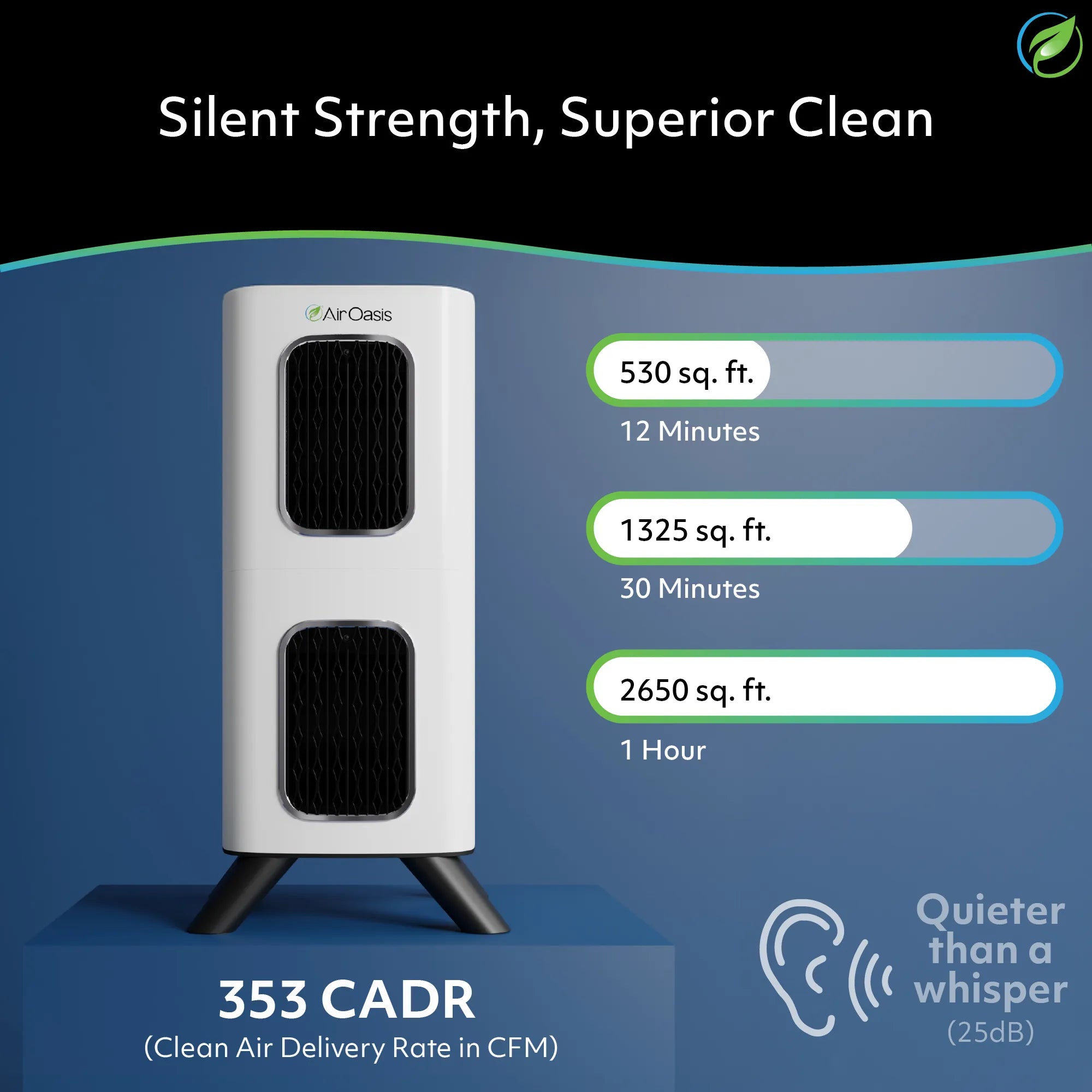
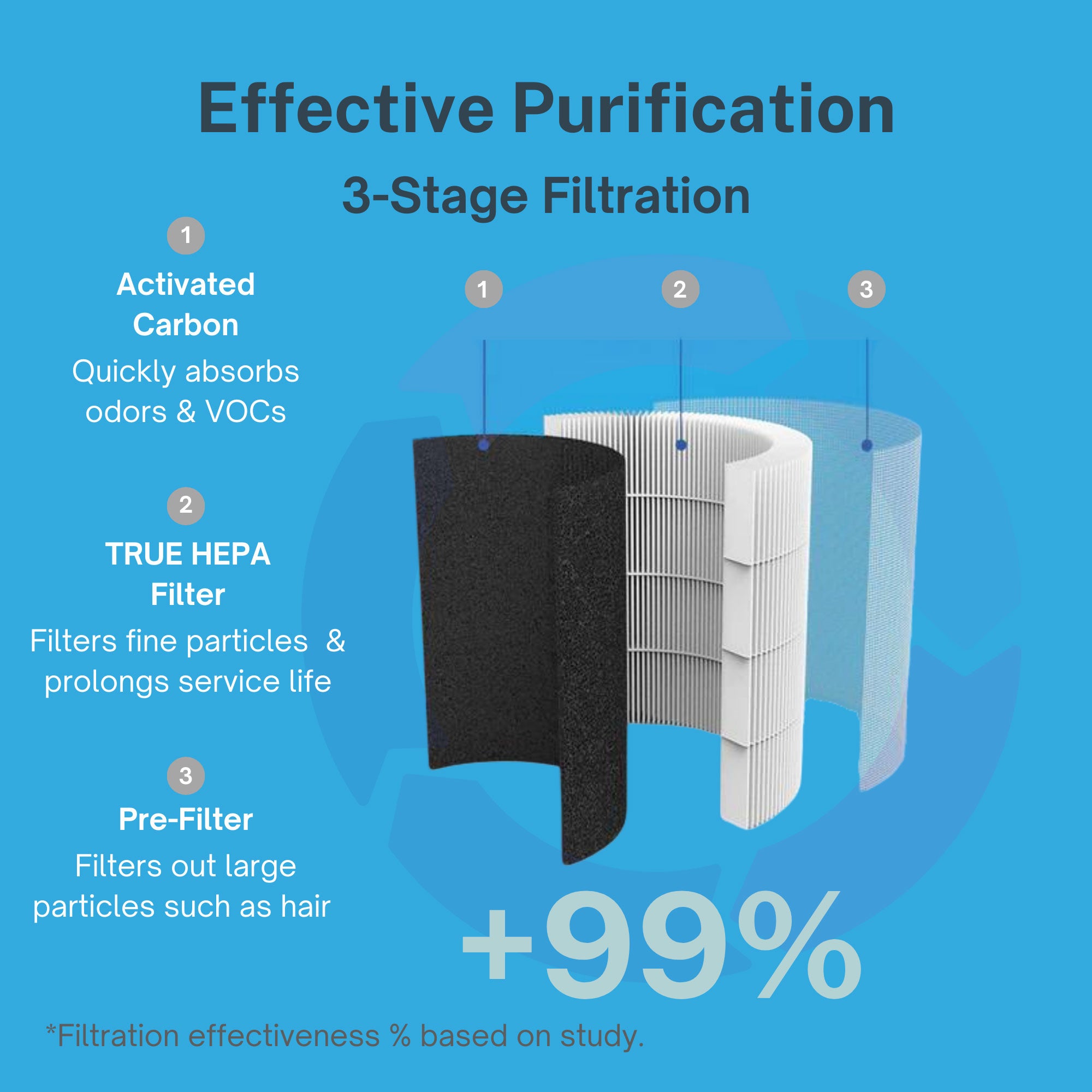
Reducing the airborne burden in your home is one concrete step in that direction. True HEPA filtration captures mold spores, mold fragments, and fine particulates that contribute to ongoing airway burden. Activated carbon addresses the microbial volatile organic compounds and other gaseous byproducts associated with water-damaged environments. For someone managing CIRS, these aren't luxuries, they're part of the baseline.
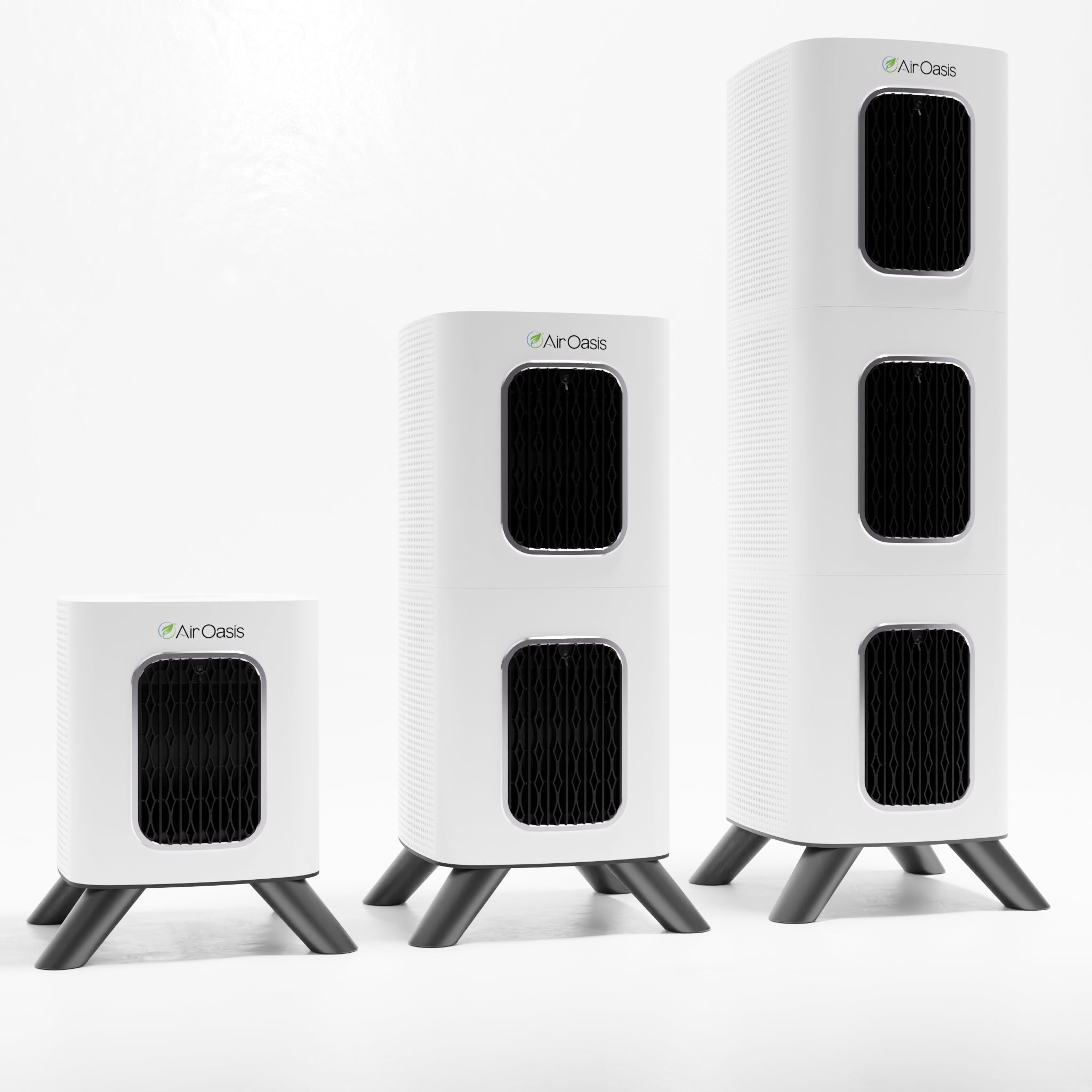
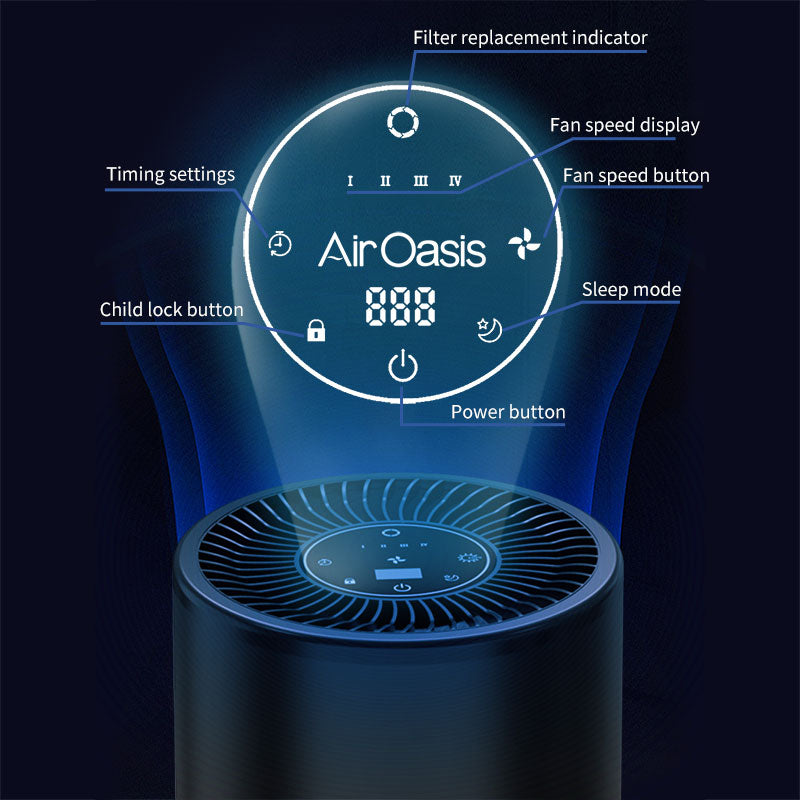
The iAdaptAir combines True HEPA filtration with activated carbon, UV-C, and bipolar ionization in a CARB-certified ozone-free unit with a removable WiFi module for those with EMF sensitivities. The 2S covers 265 square feet, the 2M covers 530, the 2L covers 795, and the 2P covers 1,059. Doors and windows closed during operation, four inches of clearance on all sides, and a unit sized for the actual room you're treating are the fundamentals.
MARCoNS is one piece of a complicated clinical picture. The framework has biological grounding, a community of physicians and patients who have found it useful, and genuine gaps in its independent research base. Understanding it honestly, without dismissing or overstating it, is the starting point for having a productive conversation with your physician. If you're working through CIRS, protecting your indoor air is something you can act on today. Shop Air Oasis, and build clean air into your recovery from the ground up. Breathe Better, Live Better.