You've done the research. You recognize your symptoms in the CIRS literature. You've spent time in a water-damaged building, maybe for years. You've seen doctors who ran standard tests and found nothing, or dismissed what you were feeling, or handed you a diagnosis that never quite fit. And now you're living in a kind of limbo, sick enough that your life has changed, but without anyone officially confirming why.
This is where a lot of people in the CIRS community actually live. Not with a confirmed diagnosis and a treatment plan, but with a strong, reasoned suspicion and no clear path to what comes next. That experience deserves a direct, honest response.
Why suspected CIRS without a formal diagnosis is so common
CIRS is not universally recognized by mainstream medicine. It has a meaningful body of peer-reviewed research behind it, most significantly the work of Dr. Ritchie Shoemaker and colleagues published across several journals, but it is not included in standard medical school curricula, and most general practitioners and even many specialists are not trained to assess for it. This is simply the current state of things, not a conspiracy, not a dismissal of patient experience.
The result is predictable. People whose symptoms fit the CIRS profile, chronic fatigue, brain fog, sleep disruption, joint pain, unusual neurological symptoms, sensitivity to light or sound, and more, often cycle through specialists for years. Each doctor addresses their particular system in isolation. Nobody connects the dots. Standard tests come back unremarkable. Patients are sometimes told their symptoms are anxiety, depression, or psychosomatic.
This is a known and documented problem. A frequently cited feature of CIRS clinical presentations is that conventional diagnostic workups typically show nothing unusual, because the relevant abnormalities, elevated C4a, TGF-β1 and MMP-9 dysregulation, suppressed alpha-MSH, VCS deficits, are not part of standard panels. If no one orders the right tests, nothing gets found.
What "suspected CIRS" actually means
Having symptoms consistent with CIRS, a history of relevant exposure, and no contradictory diagnosis is not the same thing as having confirmed CIRS. This distinction matters enormously, because the treatment protocol is specific, involves real medical interventions, and should not be self-directed based on online research alone.
That said, suspected CIRS is not nothing. It is a reasonable clinical hypothesis based on a pattern of evidence, and it is a legitimate reason to pursue further investigation with a qualified practitioner. Several things can inform whether that hypothesis is worth pursuing seriously.
The first is exposure history. CIRS, as described in the research literature, is triggered most commonly by chronic exposure to water-damaged buildings, specifically the complex mixture of mold, mycotoxins, actinobacteria, and microbial VOCs those environments produce. Other documented triggers include certain tick-borne illnesses and, according to more recent research, exposure to the SARS-CoV-2 spike protein. If there is no plausible exposure source in your history, CIRS becomes a less likely explanation for your symptoms, though this is an assessment to make with a clinician, not a reason to dismiss the possibility without looking.
The second is symptom pattern. CIRS is not a single symptom condition. The research describes a multi-system presentation affecting cognition, musculoskeletal function, neurological function, hormonal regulation, and immunity simultaneously. Fatigue alone, or brain fog alone, does not constitute a CIRS presentation. A constellation of symptoms across multiple systems, particularly in the context of a relevant exposure history, is what raises clinical suspicion appropriately.
A low-cost screening step that carries real clinical weight
One piece of the CIRS assessment that is accessible without a physician referral is Visual Contrast Sensitivity testing, or VCS. This test measures the ability of the visual system to detect gradations of contrast, a function that is impaired during the neuroinflammatory processes associated with CIRS. Failure on a validated VCS test, in the context of appropriate symptoms and exposure history, is described in the Shoemaker research as a meaningful indicator warranting further evaluation.
VCS testing is not diagnostic on its own. A failed result doesn't confirm CIRS, and a passed result doesn't rule it out. But it is an inexpensive, accessible, and clinically grounded screening step that many CIRS-aware practitioners use as part of an initial assessment. If you're trying to determine whether pursuing a formal workup is warranted, it's a reasonable place to start.
How to find a qualified practitioner
This is the piece most online resources handle poorly. The honest answer is that finding a physician who can competently assess and treat CIRS is genuinely difficult, varies significantly by geography, and requires some careful evaluation on your part.
Practitioners trained in the Shoemaker Protocol have completed specific coursework and are listed on Dr. Shoemaker's Surviving Mold website, survivingmold.com, which maintains a provider directory. This is the most commonly referenced starting point in the CIRS community and is worth using as a baseline resource.
Functional medicine practitioners and integrative physicians may have familiarity with biotoxin illness, though training and depth of experience vary considerably. When evaluating a potential practitioner, reasonable questions include whether they are familiar with the Shoemaker diagnostic criteria, whether they order the relevant biomarker panel including C4a, TGF-β1, MMP-9, and HLA-DR testing, and whether they have treated patients with confirmed CIRS previously.
Be cautious of practitioners who offer sweeping CIRS diagnoses based on symptom questionnaires alone without biomarker testing, or who recommend expensive supplement protocols in place of the published diagnostic and treatment steps. The community of people who have been financially harmed by unqualified practitioners in this space is real and worth taking seriously.
What you can do while you're still seeking answers
Living in diagnostic limbo is genuinely hard. Not having a confirmed diagnosis doesn't mean you're imagining what you're experiencing. And it doesn't mean nothing you do matters while you're pursuing answers.
The single most important environmental variable in CIRS is ongoing exposure. If you are still in or regularly returning to a water-damaged building, that is the first priority, full stop. No treatment protocol works in the presence of continued exposure. If you can leave, leave. If you cannot leave immediately, document the building's history and work toward that change as the primary goal.
Beyond removing the exposure source, managing your indoor air at home is a concrete, actionable step. Reducing the airborne burden of mold spores, fragments, and microbial VOCs in your home environment means your immune system is dealing with less, even before a formal treatment plan begins. This is not a substitute for proper medical care. It is a reasonable measure that falls within your control.
Why clean indoor air matters for this community specifically
For someone with suspected biotoxin illness, the home should be the safest air environment in their life. That's not always the default, particularly in older homes, humid climates, or buildings with any water intrusion history.
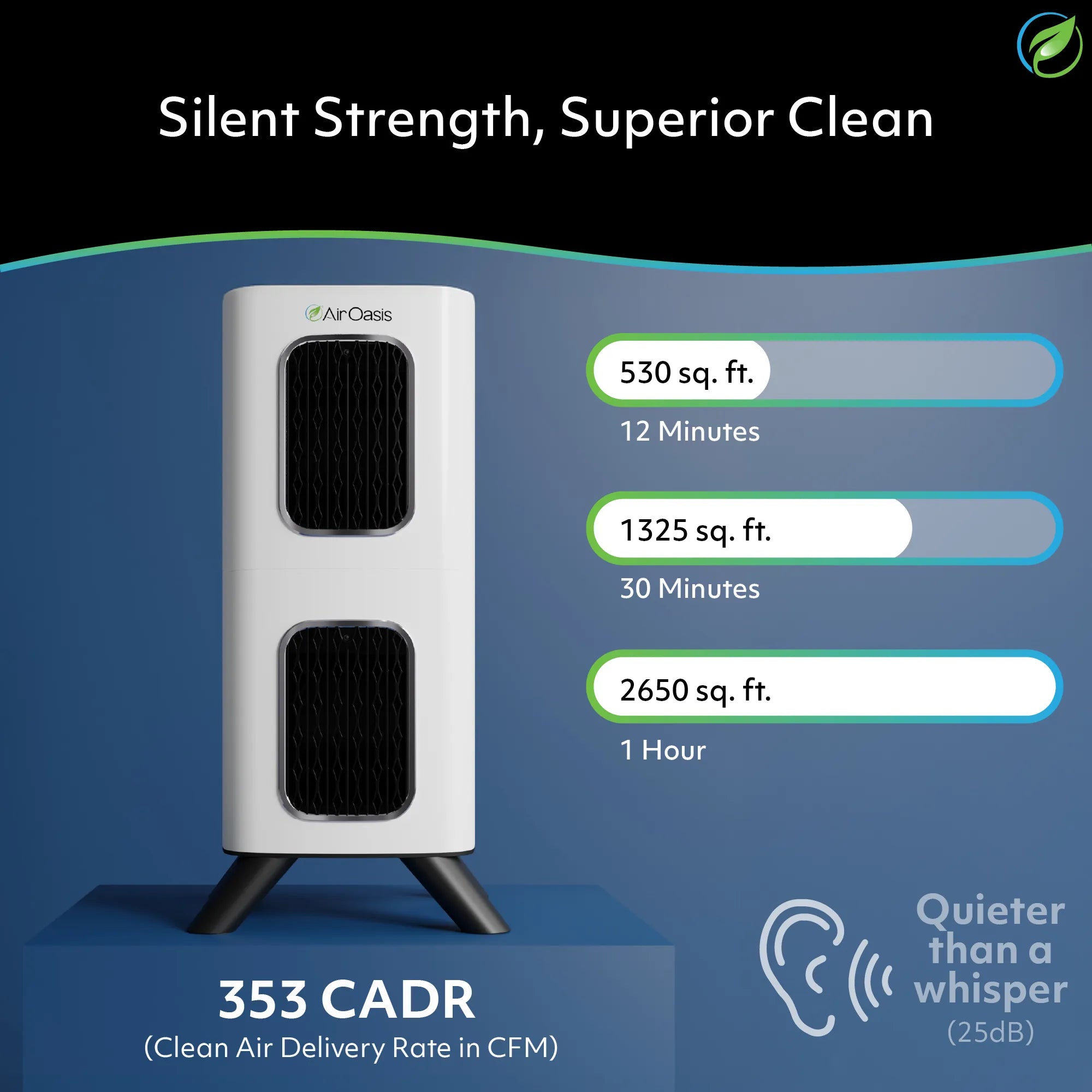
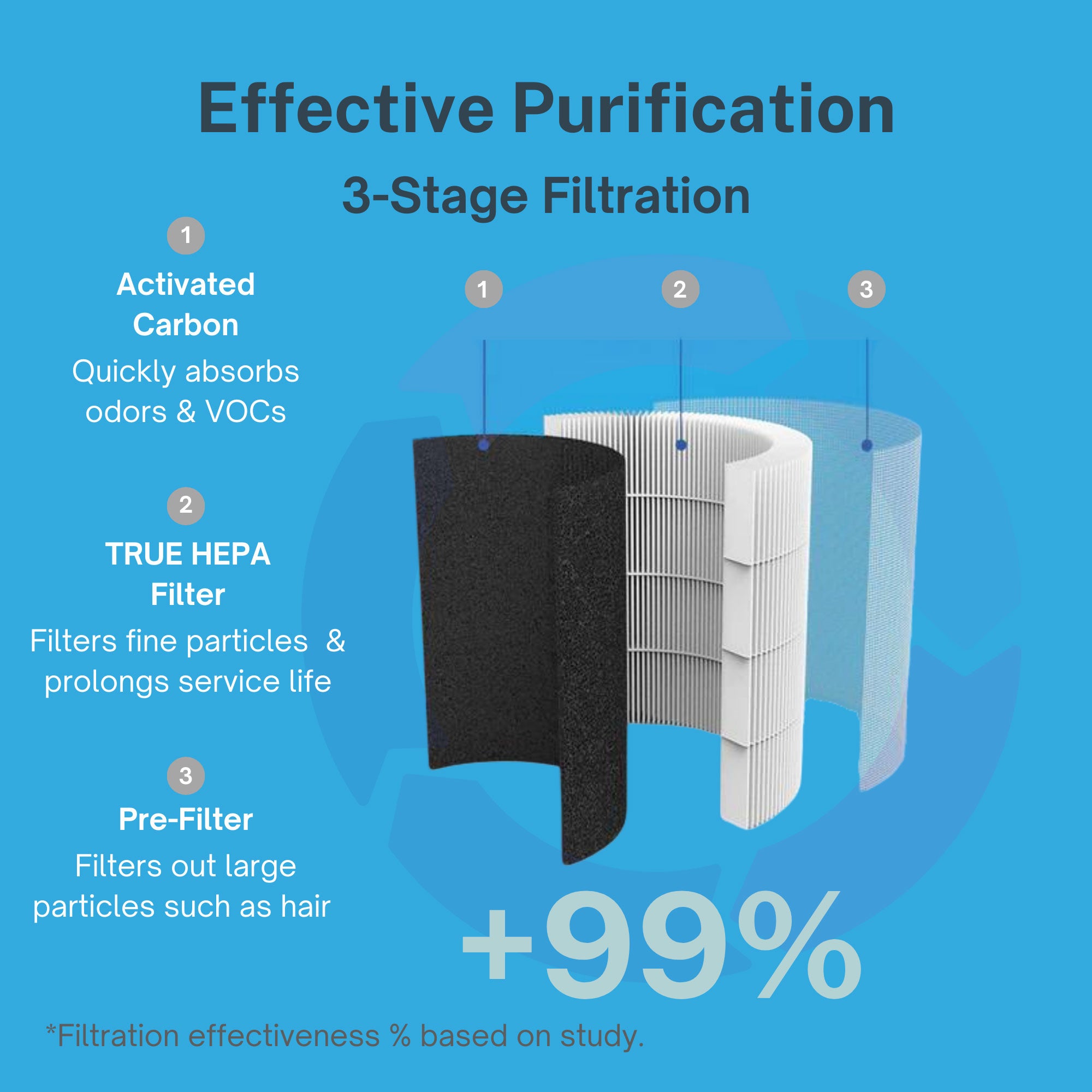
True HEPA filtration captures mold spores and fragments down to 0.3 microns. Activated carbon addresses the gaseous phase, the microbial volatile organic compounds that water-damaged environments and mold-affected materials can off-gas. Together, these two technologies address the categories of airborne exposure most relevant to biotoxin illness.
The iAdaptAir combines True HEPA, activated carbon, UV-C, and bipolar ionization in a CARB-certified ozone-free unit with a removable WiFi module for those with EMF sensitivities, a consideration the CIRS community frequently raises. For bedrooms, the 2S covers 265 square feet and the 2M covers 530. Living areas are handled by the 2L at 795 square feet or the 2P at 1,059. Doors closed during operation, four inches of clearance on all sides, and a unit matched to the actual room size are the fundamentals.
You don't need a confirmed diagnosis to take your symptoms seriously. You need accurate information, a path toward qualified assessment, and a home environment that isn't working against your recovery. Suspected CIRS is a legitimate reason to keep pushing for answers. Don't let a system that doesn't yet know how to find you become a reason to stop looking. Shop Air Oasis, and start with what you can control. Breathe Better, Live Better.