If you've been dealing with unexplained fatigue, irregular cycles, mood shifts, or sleep disruption and can't find a clear cause, it's reasonable to want to look at every variable. For women living or working in spaces with mold, the question of whether mold exposure could be contributing to hormonal symptoms is worth asking carefully, with nuance rather than alarm.
The short answer is that some research suggests a plausible connection. The longer answer requires distinguishing between what the evidence actually shows, what remains hypothetical, and what you can reasonably do about it. This article aims to give you that fuller picture.
What mycotoxins are and why they matter to this conversation
Mold is a broad category of fungi. Many molds produce compounds called mycotoxins, which are toxic secondary metabolites released during mold growth. Mycotoxins are well-established health concerns at high occupational exposures and in contaminated food supplies. Their effects at the lower concentrations typical of residential indoor mold exposure are more difficult to study and less definitively established, though research is ongoing.
What makes mycotoxins relevant to hormonal health is that some of them have been identified as endocrine disruptors. The endocrine system is the network of glands and organs that produces, stores, and releases hormones. Endocrine disruptors are substances that can interfere with that system, either by mimicking hormones, blocking hormone receptors, or altering the rate at which hormones are produced or broken down.
Laboratory research has found endocrine-disrupting activity in certain mycotoxins that are associated with common indoor molds. Ochratoxin A, produced by species in the Aspergillus and Penicillium families that can grow indoors, has shown estrogenic activity in laboratory studies, meaning it can interact with estrogen receptors in ways that may disrupt normal estrogen function. Aflatoxins have been shown to affect the hypothalamic-pituitary axis, which is the brain-based control system governing reproductive hormone production in women.
These are laboratory findings, many from in vitro or animal studies. They establish biological plausibility, meaning a credible mechanism exists for how mycotoxins could interfere with hormonal function. They do not, on their own, prove that living in a home with indoor mold will cause measurable hormonal changes in women. That distinction matters.
The hormones most likely to be involved, and what the evidence does and doesn't show
The hormonal systems most frequently discussed in the context of mycotoxin exposure include the stress hormone cortisol, reproductive hormones including estrogen and progesterone, and thyroid hormones. Here is what the research currently supports for each, stated as accurately as possible.
Cortisol and the stress response system
The hypothalamic-pituitary-adrenal axis, sometimes called the HPA axis, governs the body's cortisol production in response to perceived stress or threat, including immune threat. Mold-induced inflammation activates immune pathways that can, in turn, stimulate cortisol production. Chronic or repeated immune activation from ongoing mold exposure could theoretically place sustained demands on this system. In people diagnosed with Chronic Inflammatory Response Syndrome (CIRS), a condition associated with biotoxin exposure from water-damaged buildings, dysregulation of cortisol and other HPA axis hormones has been documented clinically. However, CIRS represents a specific, diagnosed condition affecting a subset of individuals with particular genetic susceptibilities. Whether lower-level, non-CIRS mold exposure produces meaningful cortisol dysregulation in the general population is not established by current human research.
Estrogen and progesterone
Because some mycotoxins have demonstrated estrogenic activity in laboratory settings, there is a hypothesis that indoor mycotoxin exposure could contribute to disruptions in the balance between estrogen and progesterone in women. Researchers in the menstrual cycle and indoor air quality literature have noted that no studies have yet specifically examined whether indoor mold exposure affects menstrual regularity or estrogen-progesterone balance directly in human subjects. This is described in the literature as a significant research gap. The mechanistic case for the connection is biologically plausible, but direct human evidence is currently absent.
Thyroid hormones
A review published in Frontiers in Immunology examined the association between long-term mold exposure and non-thyroidal illness syndrome, a pattern of altered thyroid hormone levels, specifically reduced T3 and T4 with elevated reverse T3, seen in the context of chronic illness and systemic inflammation. The review identified this as a potential consequence of sustained inflammatory burden from biotoxin exposure. This finding is from a clinical review in the context of chronic mold illness, not from general population studies, and applies most directly to individuals experiencing significant ongoing mold exposure.
Why the picture is complicated for women specifically
Women face a distinct hormonal context that makes the question of mold and endocrine disruption particularly relevant. The female reproductive system depends on precise, timed hormonal signaling across the menstrual cycle, during pregnancy, and through the perimenopausal transition. Systems that depend on precise timing are inherently more vulnerable to disruption than those that maintain relatively stable baseline levels.
Women who already have conditions involving hormonal dysregulation, including polycystic ovary syndrome, endometriosis, thyroid disorders, or irregular cycles, may have less resilient hormonal systems that are more susceptible to disruption from additional environmental stressors. This does not mean mold will worsen these conditions for everyone, but it does mean that women with these histories may have more reason to consider environmental contributors, including indoor air quality, when evaluating why symptoms fluctuate.
Individual susceptibility also plays a documented role in how anyone responds to mold exposure. Approximately 25% of people carry HLA-DR genetic variants that affect how efficiently the body clears biotoxins. For these individuals, even moderate mold exposure may produce more pronounced and prolonged immune and inflammatory responses, which could translate into greater potential for hormonal disruption. This genetic variability helps explain why two people living in the same home may have dramatically different responses to the same mold environment.
What symptoms might suggest an environmental hormonal connection
No symptom is specific enough to diagnose mold-related hormonal disruption on its own. Many of the symptoms associated with endocrine disruption — fatigue, sleep difficulty, mood changes, menstrual irregularity, and difficulty with concentration — have many potential causes. What might warrant a closer look at the indoor environment as one contributing factor is a pattern: symptoms that correlate with a specific space, that appeared or worsened after moving into a new home or workplace, or that improve when away from a particular building for extended periods.
If you're experiencing these kinds of symptoms and your home has a history of water damage, visible mold, a persistent musty smell, or high indoor humidity, the indoor environment is a reasonable variable to investigate, in parallel with standard medical evaluation. A physician specializing in environmental medicine or a clinician familiar with biotoxin-related illness can help evaluate whether mold exposure is a plausible contributor to your specific situation.
Addressing indoor mold: the environmental side of the equation
No intervention targeting hormonal symptoms will be fully effective if ongoing mold exposure continues. Reducing or eliminating mold in the indoor environment is the foundational step. That means addressing moisture, which is the condition mold requires to grow. Ventilation in bathrooms and kitchens, prompt repair of any plumbing leaks, humidity control to keep indoor relative humidity below 50%, and professional remediation of any confirmed mold growth behind walls or under flooring are all meaningful steps.
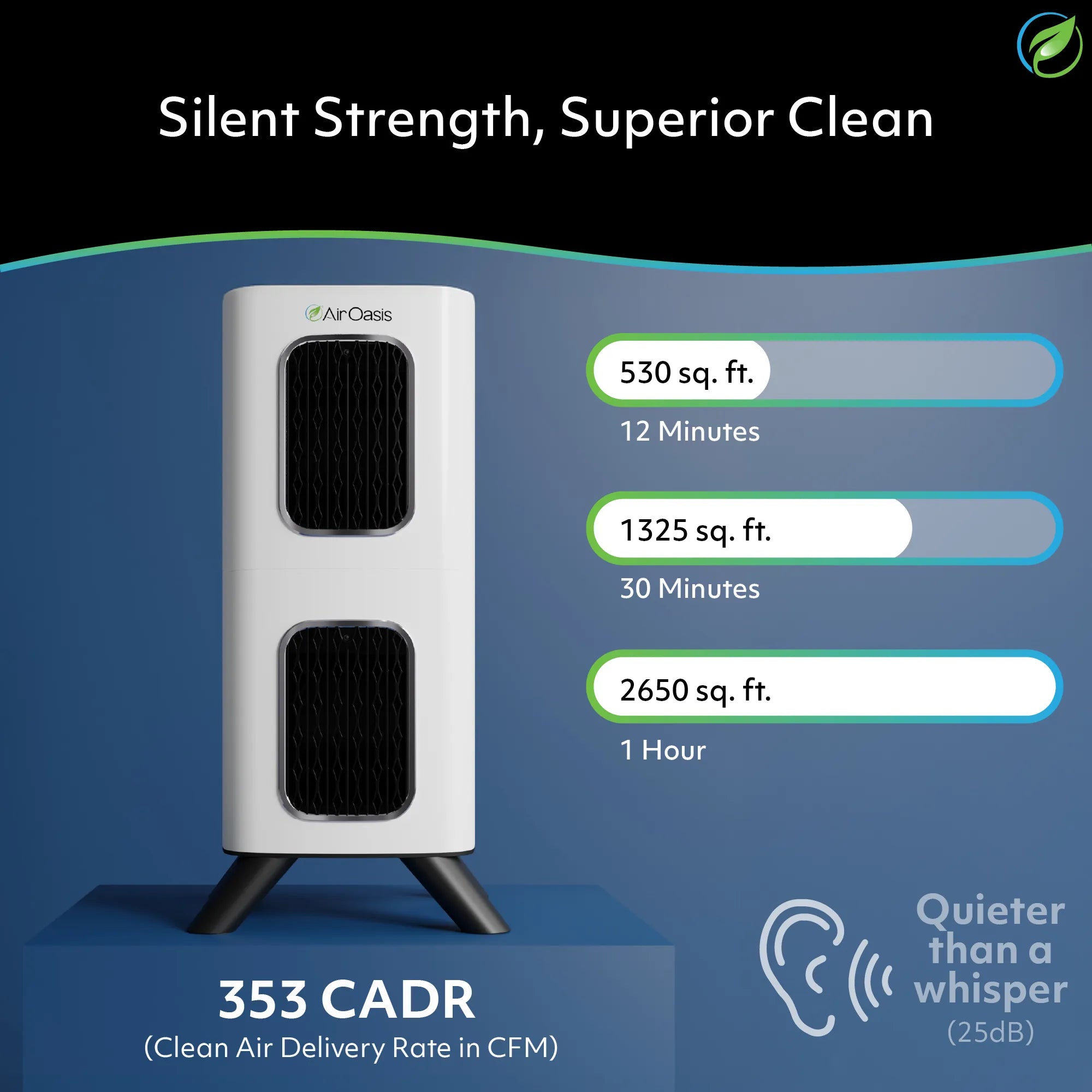
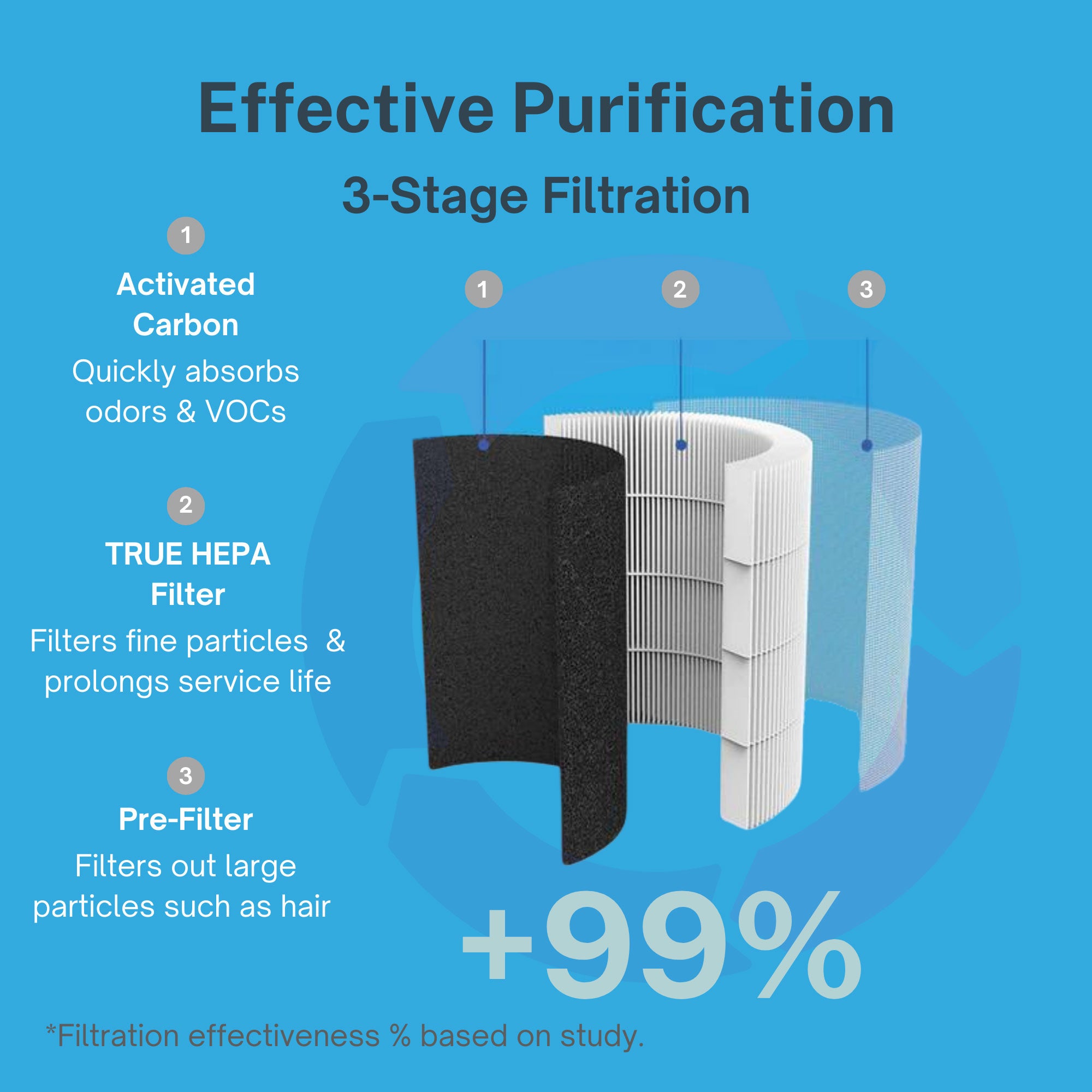
For airborne mold spores already circulating in a space, air purification provides a layer of ongoing protection. True HEPA filtration captures mold spores down to 0.3 microns, reducing the airborne load continuously. For women concerned about the cumulative effect of daily mold spore exposure, particularly in spaces they occupy for many hours, consistent filtration in the bedroom and primary living areas is a practical measure.
The iAdaptAir by Air Oasis combines True HEPA filtration with activated carbon, which addresses the microbial VOCs that mold colonies emit, alongside UV-C light and bipolar ionization. It is CARB-certified ozone-free, which matters for anyone with respiratory sensitivity or immune reactivity. Sizing the unit appropriately to the room ensures the air cycles frequently enough to maintain meaningfully lower spore concentrations. The 2S covers up to 265 square feet, the 2M covers 530 square feet, the 2L covers 795 square feet, and the 2P covers up to 1,059 square feet.
What you deserve to know going in
The research on mold exposure and hormonal health in women is at an early stage. The biological mechanisms are plausible and worth taking seriously. The direct human evidence, particularly for residential exposure levels rather than severe occupational or CIRS-level exposure, is limited. That honest picture is worth holding onto as you evaluate your own situation, because it means neither dismissing your concerns nor drawing conclusions beyond what the evidence supports.
What is clear is that reducing mold exposure is a reasonable, evidence-supported step for anyone living with indoor mold, regardless of what future research shows about hormonal effects specifically. If you're ready to address your indoor air environment, Shop Air Oasis and find the iAdaptAir model sized for your space.