If you have Chronic Inflammatory Response Syndrome, you already know that sleep is one of the first things to go wrong. Not just in quantity, but in quality. You may sleep eight hours and wake up feeling worse than when you went to bed. You may lie awake while exhausted, your system running too hot even as your body desperately needs rest. Sleep problems in CIRS are real, documented, and rooted in specific physiological disruptions. The question of whether sleep position plays any role in how severe those symptoms feel is more nuanced, and it deserves a careful answer.
How CIRS disrupts sleep at a biological level
To understand whether sleep position could matter, you first need to understand why sleep is so compromised in CIRS to begin with.
CIRS is a multi-system inflammatory illness that develops in genetically susceptible individuals, roughly 25 percent of the population carrying HLA-DR variants, who are unable to efficiently clear biotoxins from mold, bacteria, or other sources. The resulting chronic immune activation drives persistent systemic inflammation that affects the nervous system, hormone regulation, and brain function.
Several specific mechanisms are understood to disrupt sleep in CIRS. One is dysregulation of the HPA axis, the hypothalamic-pituitary-adrenal system that governs the stress response and interacts closely with circadian rhythm. When the inflammatory state keeps the immune system activated, the stress response remains active. The body interprets ongoing internal inflammation as a signal that it is not safe to rest. This produces the characteristic wired-but-exhausted state many CIRS patients describe, physiological arousal that blocks sleep onset even when fatigue is severe.
A second mechanism involves melanocyte-stimulating hormone, or MSH. This regulatory hormone, which helps govern inflammation, circadian rhythm, gut barrier integrity, and mood, is typically deficient in CIRS patients. MSH plays a role in promoting restful, restorative sleep. Its deficiency in CIRS contributes to disrupted sleep architecture, with reduced slow-wave and REM sleep, frequent nighttime waking, and sleep that does not feel restorative regardless of duration.
Third, neuroinflammation from biotoxin-driven immune activation affects the neurotransmitter systems that regulate sleep, including serotonin, dopamine, and GABA pathways. Disruption to these systems can produce insomnia, anxiety at night, and sleep that is fragmented rather than continuous.
These mechanisms are documented in the CIRS literature and represent real physiological disruption, not simply sleep hygiene problems that can be resolved by going to bed at the same time each night.
What the research does and does not say about sleep position and CIRS
Here is the honest answer to the central question: there is no published research, as of this writing, that has directly studied whether sleep position affects CIRS symptom severity. None. The question has not been formally investigated in this population.
What that means is that any claim connecting sleep position specifically to CIRS outcomes would be extrapolation rather than evidence. It would be going beyond what the science actually says. That matters enormously for a community that has already been subject to a great deal of misinformation, dismissal, and unsupported health claims.
What can be discussed are areas where established sleep-position research intersects with problems that CIRS patients commonly experience, with the clear understanding that these are general findings applied by inference to CIRS, not direct evidence.
Sleep position, nasal congestion, and upper airway function
Nasal and sinus congestion is a documented symptom among many CIRS patients, and it intersects with a well-established area of sleep-position research. Sleeping on one's side tends to improve nasal airflow compared to sleeping on the back in people with congestion, because supine positioning can worsen nasal resistance and post-nasal drip. For CIRS patients with significant sinus symptoms, this is a general principle worth knowing, though it is not CIRS-specific research.
Obstructive sleep apnea, which is worsened by supine sleep position in many people, also disrupts sleep architecture and produces non-restorative sleep with daytime fatigue. Given the overlapping symptom profile between sleep apnea and CIRS, particularly fatigue, brain fog, and unrefreshing sleep, clinicians familiar with CIRS recommend ruling out sleep apnea as a concurrent or confounding diagnosis. Sleep position may be one relevant factor if apnea is present.
Sleep position and glymphatic clearance: promising but not proven in CIRS
One area of sleep science that has generated significant interest in the context of neurological conditions is the glymphatic system. This is the brain's waste-clearance system, which operates primarily during sleep, flushing cerebrospinal fluid through brain tissue to remove metabolic byproducts and inflammatory compounds. A 2019 study by Lee et al. published in the Journal of Neuroscience suggested that lateral sleep position may favor glymphatic clearance compared to supine or prone positioning, at least in animal models.
This finding is preliminary and based primarily on animal studies. Whether it translates to meaningful differences in humans remains under active investigation. Whether glymphatic clearance is specifically impaired in CIRS, and whether optimizing sleep position could improve it in this population, has not been studied. The hypothesis is scientifically plausible given what is known about neuroinflammation in CIRS and the role of the glymphatic system in clearing inflammatory compounds from brain tissue, but plausible is not the same as demonstrated.
If you have CIRS and you are curious about sleep position, lateral positioning is generally considered reasonable for overall sleep health, and it carries no known risks. But it should not be presented or understood as a CIRS treatment, and it will not address the underlying mechanisms, HPA axis dysregulation, MSH deficiency, and neuroinflammation, that drive sleep disruption in this illness.
What actually helps with CIRS-related sleep disruption
The evidence-based approaches to sleep disruption in CIRS are grounded in addressing the underlying inflammatory and hormonal mechanisms, not in sleep optimization techniques alone.
The single most important step is removing ongoing biotoxin exposure. The inflammatory cascade that disrupts sleep cannot resolve while exposure continues. This means leaving the water-damaged environment and, where possible, living and sleeping in a space with low mold spore and mycotoxin burden. This is not a simple step for many people with CIRS, but it is the foundational one.
Beyond removal from exposure, working with a physician experienced in CIRS to address MSH deficiency, HPA axis dysregulation, and associated hormonal imbalances is the clinical pathway that addresses sleep disruption at its root. Standard sleep hygiene practices, limiting blue light, consistent sleep timing, reducing stimulation before bed, may offer modest supportive benefit, but they are unlikely to restore restorative sleep while the underlying inflammation is active.
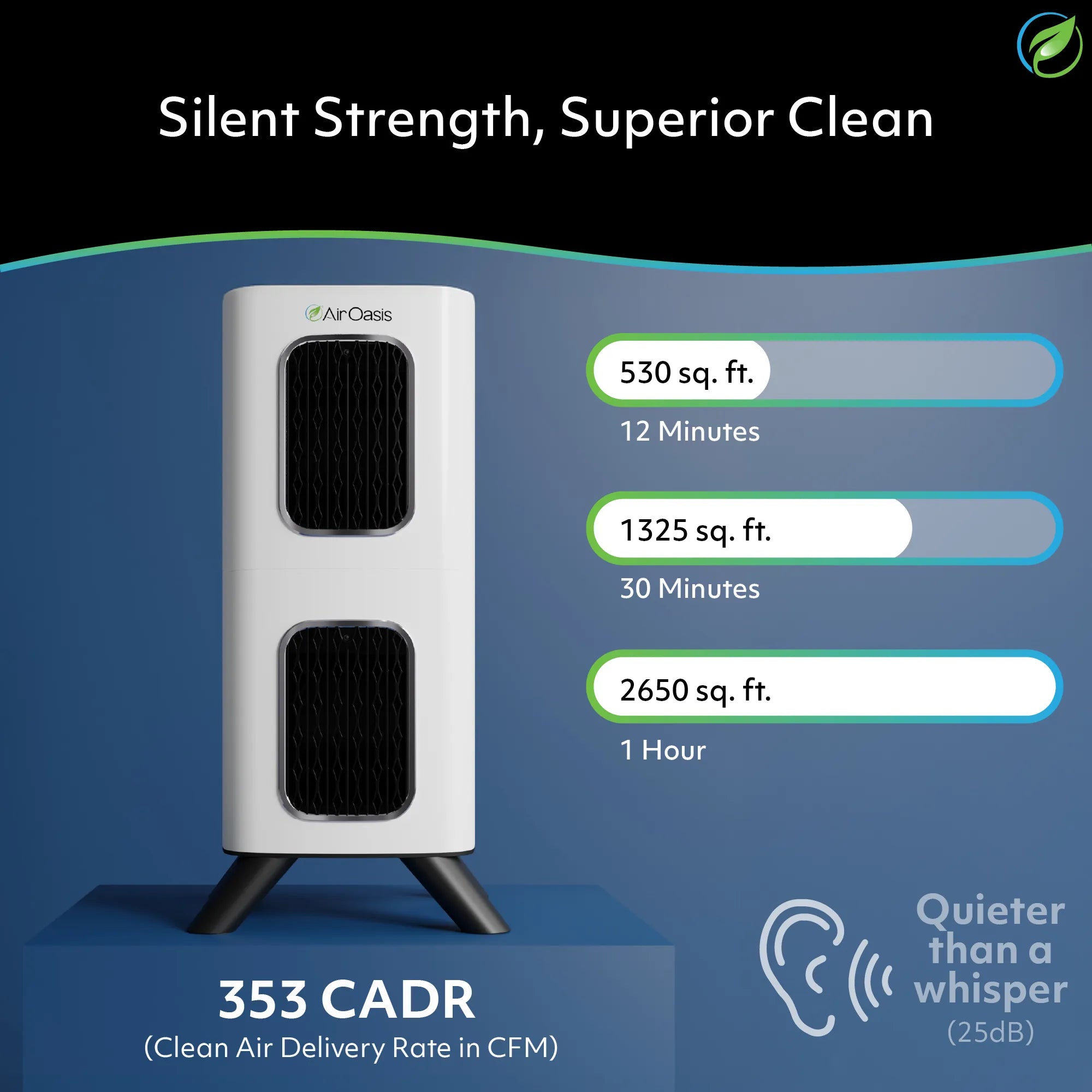
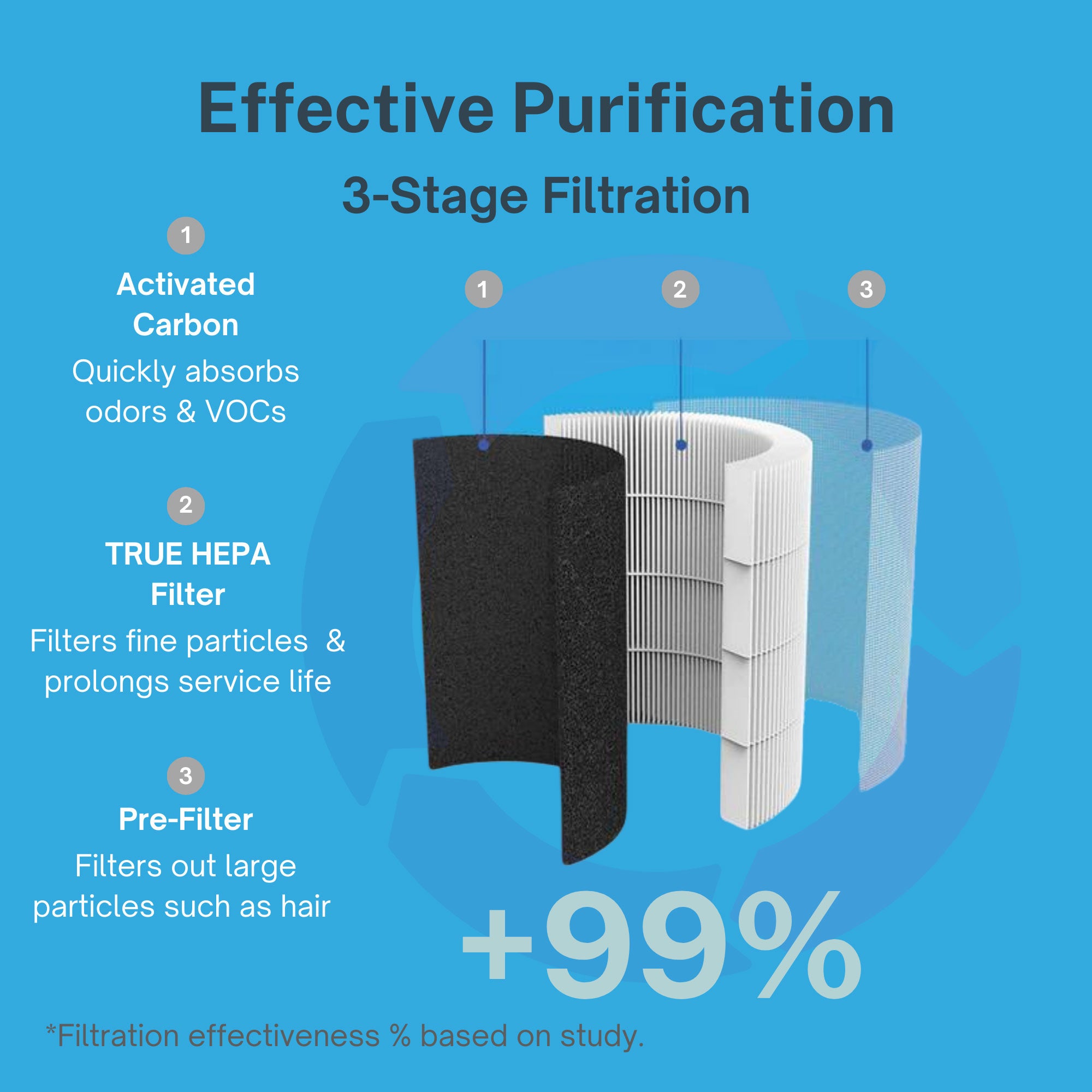
The air quality of the bedroom matters significantly during recovery. Mold spores, mycotoxin-associated particulates, and VOCs from water-damaged materials can sustain low-level exposure even after a person has left the primary contaminated environment, particularly if belongings or materials from that environment have been brought into the home. True HEPA filtration captures airborne mold spores and fine particulates down to 0.3 microns. Activated carbon addresses the volatile organic compounds associated with mold-affected materials.
The iAdaptAir combines both technologies with UV-C light and bipolar ionization in a CARB-certified ozone-free unit appropriate for continuous overnight operation in bedrooms. For someone in CIRS recovery, the bedroom environment where they spend hours each night is one of the highest-priority spaces to protect. The iAdaptAir 2S covers up to 265 sq ft, appropriate for most bedrooms. The 2M covers up to 530 sq ft for larger spaces. Maintain four inches of clearance on all sides, keep the door closed during operation, and keep the unit out of direct sunlight.
Sleep position is a reasonable question without a proven answer
It is entirely reasonable for people with CIRS to wonder whether something as simple as how they sleep might influence how they feel. The question comes from a good place and reflects the kind of careful attention to their own bodies that many CIRS patients have had to develop precisely because mainstream medicine has often missed what was happening to them.
The honest answer today is that sleep position has not been studied specifically in CIRS. What is known about sleep position and general sleep health, glymphatic function, and nasal airway physiology may be relevant to CIRS patients, but it remains extrapolation rather than evidence. Work with a qualified practitioner, remove yourself from exposure, protect the air in your sleeping environment, and address the underlying mechanisms. That is where the evidence points.
Shop Air Oasis for ozone-free air purification built for the sensitivity level that CIRS recovery demands. Breathe Better, Live Better.