Your doctor diagnosed you with Chronic Inflammatory Response Syndrome from mold exposure. Now you're wondering—could this biotoxin illness also be harming your kidneys? The answer remains frustratingly unclear due to limited research in this area.
What We Actually Know About Mold and Kidneys
Research clearly establishes that certain mold toxins can damage the kidneys. However, the specific connection between CIRS as a syndrome and chronic kidney disease remains largely unexplored. This represents a significant gap in medical knowledge that deserves attention.
Ochratoxin A stands out as the most studied kidney-toxic mycotoxin. This toxin comes from Aspergillus and Penicillium molds commonly found in contaminated grains, coffee, wine, dried fruits, and some nuts. Studies document that ochratoxin A causes oxidative stress, damages kidney tubules, and triggers chronic inflammation in kidney tissues.
The mechanism involves direct toxic effects on kidney cells. Ochratoxin A accumulates in kidney tissue over time with repeated exposure. It generates reactive oxygen species that overwhelm cellular defenses. The resulting oxidative damage affects kidney function progressively. Chronic interstitial nephritis develops as inflammation persists.
Aflatoxins represent another group of nephrotoxic mycotoxins. These come from Aspergillus molds growing on grains, nuts, and seeds. While aflatoxins are better known for liver toxicity, they also affect the kidneys through oxidative stress and inflammatory pathways. However, aflatoxin exposure differs from typical indoor mold situations that trigger CIRS.
The Missing Research Connection
Here's the critical problem—most CIRS research focuses on neurological, hormonal, and respiratory effects. Kidney function testing rarely appears in CIRS diagnostic protocols. The standard Shoemaker Protocol doesn't routinely monitor kidney markers beyond basic metabolic panels.
This creates a knowledge blind spot. We cannot definitively say whether CIRS patients experience higher rates of kidney disease because nobody has systematically studied this question. The absence of research doesn't mean no connection exists. It simply means we lack data to make informed conclusions.
CIRS involves chronic systemic inflammation affecting multiple organ systems. The kidneys filter blood continuously and face exposure to circulating inflammatory molecules. Logically, prolonged inflammation might affect kidney function. However, logic alone cannot substitute for actual clinical research.
The genetic component of CIRS adds another layer of complexity. Approximately 25% of people carry HLA-DR gene variants, preventing efficient biotoxin clearance. These individuals experience prolonged inflammatory responses. Whether this genetic susceptibility also increases kidney vulnerability to toxin damage remains completely unknown.
What Kidney Experts Say About Toxins
Recent nephrology research highlights environmental toxins as overlooked contributors to chronic kidney disease. A comprehensive review identified multiple nephrotoxic exposures, including heavy metals, mycotoxins, pesticides, and air pollution. Ochratoxin A specifically appeared on this list of concerning environmental kidney toxins.
The review noted that toxin-related kidney damage often goes unrecognized. Standard kidney disease risk factors like diabetes and hypertension receive primary attention. Environmental exposures get minimal consideration during diagnosis. This mirrors how CIRS itself frequently goes undiagnosed or misdiagnosed.
Patients taking immunosuppressant medications face a particularly high risk from mold toxins. Transplant recipients and people with autoimmune diseases taking these drugs show impaired toxin clearance. Their compromised immune systems cannot effectively eliminate mold compounds. This increases toxic accumulation and potential kidney damage.
However, these observations about mycotoxin kidney toxicity come from general environmental medicine research—not from studies specifically examining CIRS patients. The distinction matters because CIRS involves unique inflammatory patterns and genetic susceptibilities not addressed in broad environmental health studies.
Indirect Mechanisms of Potential Harm
Even without direct research, we can identify plausible mechanisms through which CIRS might affect the kidneys. Chronic systemic inflammation damages blood vessels throughout the body. Kidneys contain extensive vascular networks that filter massive blood volumes daily. Inflammatory damage to kidney blood vessels could impair filtration function over time.
The hormone disruptions in CIRS might secondarily affect kidneys. Low vasopressin (ADH) causes frequent urination and dehydration in CIRS patients. Chronic dehydration stresses kidneys. Cortisol dysregulation affects fluid balance and blood pressure—both critical for kidney health. These hormonal imbalances create conditions potentially harmful to kidney function.
VEGF deficiency commonly occurs in CIRS. Vascular endothelial growth factor maintains healthy blood vessel function including kidney vasculature. Low VEGF reduces blood flow to small vessels throughout the body. Reduced kidney blood flow could theoretically impair kidney function, though this specific connection hasn't been studied in CIRS patients.
Medication exposures complicate the picture. Many CIRS patients try multiple medications and supplements before receiving proper diagnosis. Some take cholestyramine or Welchol long-term as part of treatment. While these bile acid sequestrants primarily work in the intestines, their effects on kidney function in CIRS patients remain unexamined.
The Inflammation Connection
Both CIRS and chronic kidney disease involve persistent inflammation. Inflammatory cytokines circulate systemically in CIRS patients. Studies document elevated C4a, TGF-β1, and MMP-9 in CIRS. These same inflammatory markers appear in various kidney diseases.
Transforming growth factor beta-1 particularly deserves attention. This cytokine drives fibrosis—scarring of tissues. Kidney fibrosis represents a common pathway to chronic kidney disease regardless of the initial cause. Elevated TGF-β1 in CIRS theoretically could promote kidney fibrosis, but nobody has investigated whether this actually occurs.
Matrix metalloproteinase-9 also raises questions. This enzyme breaks down the extracellular matrix in tissues. Elevated MMP-9 appears in both CIRS and kidney disease. However, whether CIRS-related MMP-9 elevation specifically damages kidney tissue remains purely speculative without supporting research.
The challenge involves distinguishing correlation from causation. Inflammation exists in both conditions. This doesn't prove CIRS causes kidney problems. Many inflammatory conditions don't significantly affect the kidneys. We cannot draw conclusions without proper studies.
What CIRS Patients Should Know
Given the lack of specific research, what should CIRS patients do about potential kidney concerns? Reasonable monitoring makes sense even without definitive evidence. Basic kidney function testing costs little and provides valuable baseline information.
Request serum creatinine and blood urea nitrogen testing at CIRS diagnosis. Calculate your estimated glomerular filtration rate (eGFR). These standard tests assess overall kidney function. Repeat them annually or more frequently if results show abnormalities.
Urinalysis provides additional information. Protein in urine signals potential kidney damage. Blood in urine warrants investigation. These simple tests detect early kidney problems before symptoms appear. Early detection enables intervention before permanent damage occurs.
Stay well hydrated despite frequent urination from low ADH. Dehydration stresses kidneys unnecessarily. Adequate fluid intake helps kidneys function optimally even under inflammatory stress. Your urine should remain light yellow rather than dark or concentrated.
Avoid additional nephrotoxic exposures when possible. Limit NSAID use. Minimize exposure to pesticides and air pollution. Reduce dietary sources of heavy metals and mycotoxins. These precautions benefit everyone, but especially matter for people with existing inflammatory conditions.
The Need for Future Research
The medical community needs systematic studies examining kidney function in CIRS patients. Such research should include baseline kidney testing at diagnosis, longitudinal monitoring during treatment, and comparison to matched controls without CIRS.
Researchers should investigate whether genetic CIRS susceptibility correlates with kidney disease risk. Do HLA-DR gene variants that impair biotoxin clearance also increase kidney vulnerability? This question deserves investigation, given the kidneys' role in filtering and eliminating toxins.
Studies should examine whether successful CIRS treatment improves kidney function in patients with both conditions. If reducing inflammation and eliminating biotoxins helps kidney markers normalize, this would support a causal connection. Lack of improvement wouldn't disprove a connection but would provide useful information.
Protecting Kidney Health With CIRS
Until research provides clearer answers, CIRS patients should take reasonable kidney protective measures. Clean indoor air quality reduces ongoing biotoxin exposure that might theoretically harm kidneys. Medical-grade air purification removes mold spores and fragments.
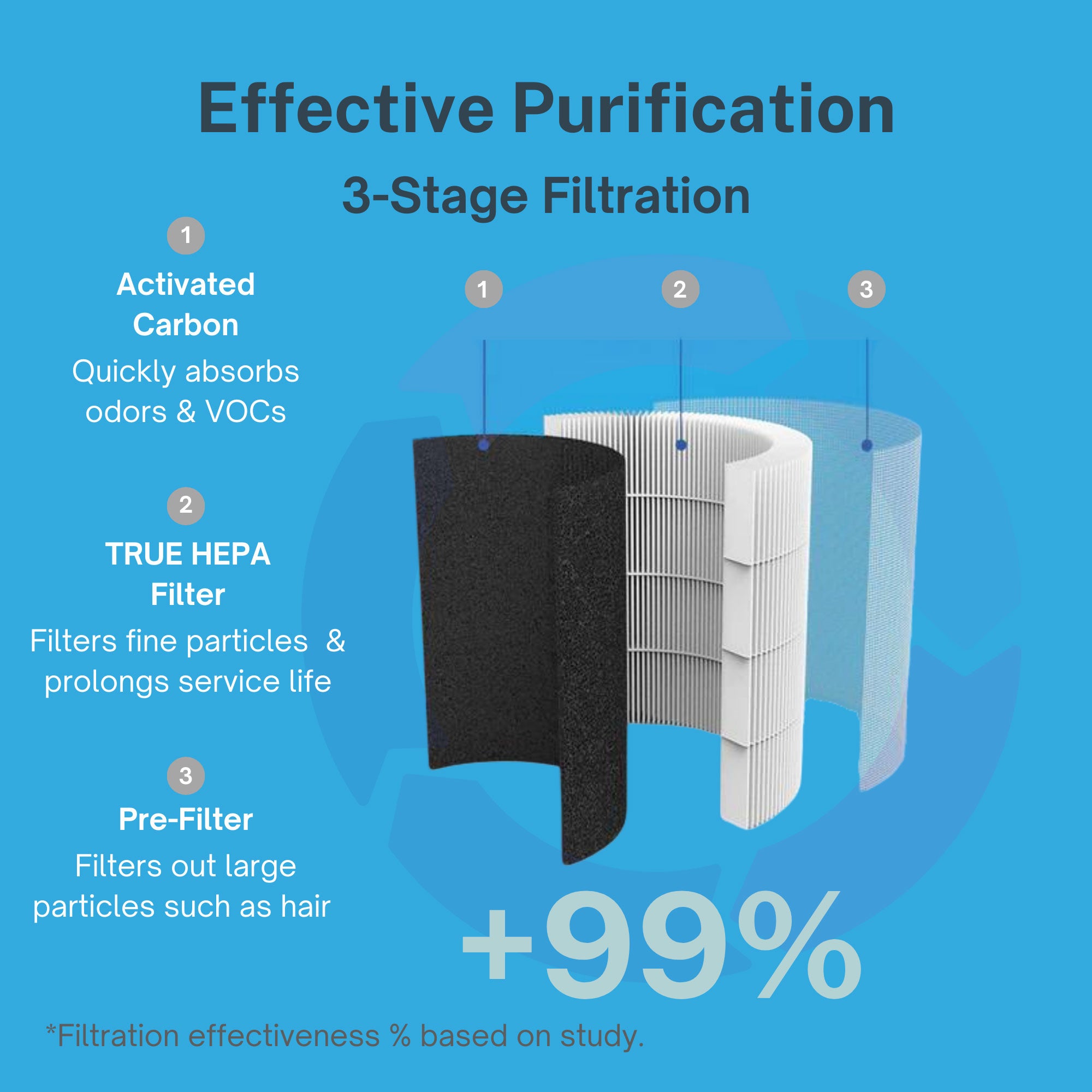
The iAdaptAir series provides comprehensive mold protection. HEPA filtration captures 99.97% of mold spores down to 0.3 microns. Activated carbon removes volatile organic compounds from mold growth. Multi-stage filtration including UV-C light inactivates airborne microorganisms that produce mycotoxins.
Choose appropriate coverage for your space. The iAdaptAir 2S purifies 265 sq ft, the 2M handles 530 sq ft, the 2L covers 795 sq ft, and the 2P serves 1,059 sq ft. Complete home air purification reduces total biotoxin burden, potentially benefiting all organ systems, including the kidneys.
The Bottom Line on CIRS and Kidneys
Current evidence cannot definitively answer whether CIRS causes or contributes to chronic kidney disease. Certain mold toxins clearly harm the kidneys. CIRS involves systemic inflammation and toxin exposure. However, specific research examining kidney function in CIRS patients simply doesn't exist.
This knowledge gap doesn't mean CIRS patients should ignore kidney health. Reasonable monitoring and protective measures make sense given what we know about mycotoxins, inflammation, and kidney disease from other contexts. Future research will hopefully clarify this important question.
Protect yourself from ongoing mold exposure regardless of kidney concerns. Clean indoor air benefits your entire body. Shop Air Oasis today and eliminate the biotoxin exposure driving your CIRS symptoms.