For most people, exercise is straightforwardly good advice. It builds strength, supports cardiovascular health, improves sleep, and lifts mood. So when a CIRS patient is told by their practitioner to hold off on starting a workout routine, it can feel counterintuitive — even discouraging. But the physiology of Chronic Inflammatory Response Syndrome creates specific conditions in which exercise, particularly when introduced too early or too intensely, can make recovery significantly harder rather than easier.
What CIRS Does to the Body's Energy Systems
Chronic Inflammatory Response Syndrome is characterized by an ongoing inflammatory process that, among its many effects, impairs circulation in the smallest blood vessels — the capillaries. This reduced capillary perfusion limits the amount of oxygen delivered to tissues throughout the body, including muscle tissue.
Under normal circumstances, muscles use oxygen efficiently to produce energy during physical activity. When oxygen delivery is compromised, muscles reach what is called the anaerobic threshold — the point at which the body can no longer sustain energy production through aerobic (oxygen-dependent) pathways — much sooner than it would in a healthy person. Once that threshold is crossed, the body shifts to less efficient energy pathways, and protein begins to be broken down into amino acids to compensate. Glycogen stores — the secondary energy reserve normally held in muscle tissue — are depleted rapidly and with poor efficiency. The result is pronounced fatigue, muscle cramping, and shortness of breath, sometimes from activity as modest as climbing a short flight of stairs.
This is not a matter of fitness level or motivation. It reflects a physiological constraint imposed by the inflammatory process itself.
The Push-and-Crash Pattern
CIRS patients often describe a pattern that clinicians working in this space refer to as "push and crash." On a day when symptoms feel manageable, a patient attempts more physical activity than their system can currently sustain. The effort feels possible in the moment — but within hours, or by the following day, fatigue and muscle soreness return severely, sometimes lasting several days.
This cycle is discouraging and can set back recovery. It also reinforces why the timing and structure of any exercise program matter so much for this population. Attempting exercise that exceeds the current anaerobic threshold — even once — can trigger a setback that takes days to recover from. This is why clinical guidance specific to CIRS emphasizes that exercise should not be introduced until the patient has reached an appropriate stage in their recovery, and only then in a carefully graduated structure.
When and How Exercise Can Be Reintroduced
The Shoemaker Protocol — the most widely referenced clinical framework for CIRS diagnosis and treatment — provides specific exercise guidelines designed around the physiological realities described above. These guidelines are intended to be implemented under the oversight of a CIRS-trained practitioner, who can assess a patient's recovery status and tailor recommendations accordingly.
The general framework begins with just five minutes of low-intensity activity — walking or a stationary bike with no incline or resistance. If that is tolerated without setback, two minutes are added daily until the patient can sustain fifteen minutes. Only after that baseline is established does light muscle training begin, starting with abdominal exercises at no more than five minutes, then gradually expanding to additional muscle groups. Resistance is not added until a full 45-minute program of combined cardio and muscle work is tolerated comfortably.
The rationale for this incremental approach involves a hormone called adiponectin, which regulates fat metabolism and helps muscles access fatty acids as an energy source. Daily incremental increases in activity are thought to gradually raise adiponectin levels, improving the energy available to muscles over time. The protocol emphasizes that skipping even a single day can slow progress meaningfully — consistency at low intensity outperforms intermittent effort at higher intensity.
The important caveat is that none of this begins until the patient is at an appropriate recovery stage, as determined by their practitioner. Starting an exercise program before the body is ready — regardless of how gentle — is unlikely to help and may hinder recovery.
Re-Exposure Remains the Core Variable
A crucial point for any CIRS patient experiencing worsening symptoms — whether during exercise attempts or otherwise — is that continued biotoxin exposure is the most common reason for lack of progress or deterioration. If the home or work environment contains ongoing mold contamination, the inflammatory process driving the physiological impairments described above is continuously being fed. No recovery protocol, including carefully managed exercise, can make meaningful headway against an active exposure source.
This is why environmental assessment is considered foundational in the Shoemaker Protocol. ERMI or HERTSMI-2 testing of the home environment is recommended to confirm the space is safe before assuming that symptoms represent a recovery plateau rather than ongoing exposure. A CIRS patient who has done everything right clinically but remains in a water-damaged building will not recover — and symptom worsening during any physical exertion should prompt reassessment of the environment, not just the exercise protocol.
The Role of Indoor Air Quality in CIRS Recovery
Maintaining the lowest possible airborne mold spore and mycotoxin load in the home is a cornerstone of CIRS environmental management. Mold spores are microscopic and remain suspended in indoor air for extended periods; even a properly remediated home can have ongoing spore infiltration from outdoor sources, HVAC systems, or materials that weren't fully addressed during remediation.
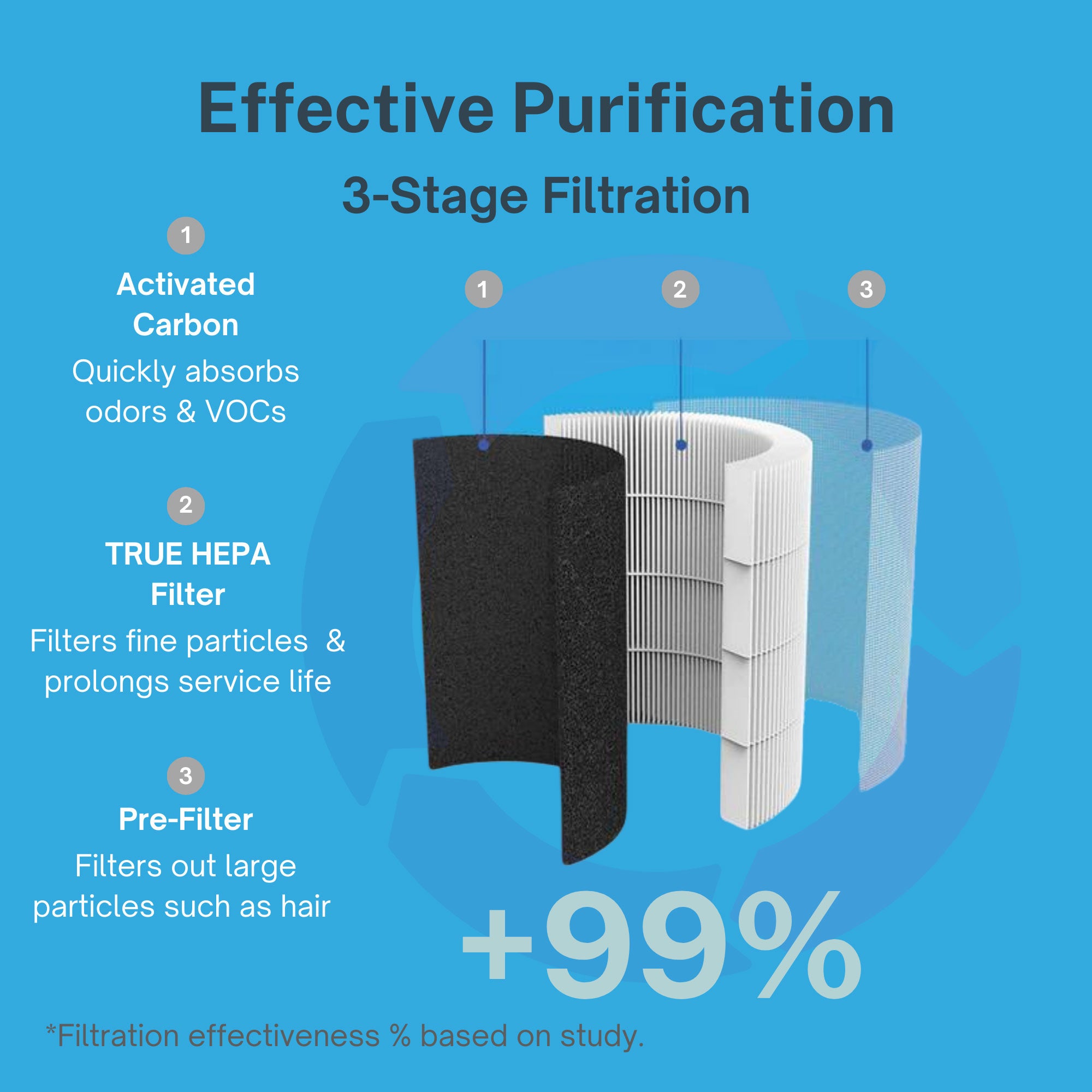
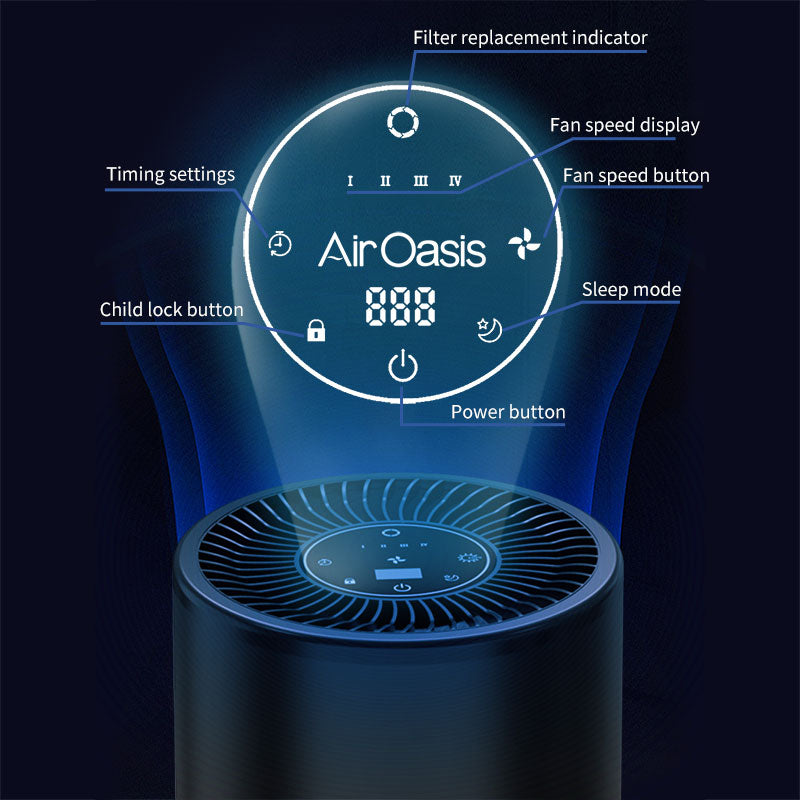
The iAdaptAir by Air Oasis is recommended by CIRS specialists, including Dr. Ritchie Shoemaker, as part of the environmental management approach for biotoxin illness. Its True HEPA filtration captures mold spores and fine particles at 0.3 microns. Activated carbon addresses mycotoxin-laden VOCs. UV-C light and bipolar ionization provide additional layers of protection. The removable WiFi module accommodates the EMF sensitivities that many CIRS patients report. It is CARB-certified ozone-free — an important consideration for patients whose systems are already under inflammatory stress.
Recovery Requires Patience, Precision, and a Clean Environment
Exercise is not the enemy for CIRS patients — but timing, intensity, and progression are everything. Pushing beyond what the body can currently sustain physiologically doesn't build resilience in CIRS; it depletes it. The path back to physical capacity runs through a careful, graduated approach guided by a knowledgeable practitioner, a confirmed safe living environment, and steady, patient progress. Shop Air Oasis today and support your recovery with the cleanest possible air at home.