If you're managing CIRS, you've probably already heard about intermittent fasting. It's everywhere in the chronic illness community, touted for its anti-inflammatory effects and its potential to support cellular cleanup processes. And the questions are reasonable: could structured fasting reduce the systemic inflammation that defines CIRS? Could it help the body clear biotoxin-related burdens? Or could fasting stress an already taxed system and make things worse?
Here is the most honest answer available in 2026: no clinical research directly examines intermittent fasting in CIRS populations. That's not a gap easily glossed over. It's the central fact that should shape how you approach this topic.
What CIRS is and why nutrition questions are genuinely complicated
CIRS (Chronic Inflammatory Response Syndrome) is a multi-system illness triggered by biotoxin exposure, most commonly from water-damaged buildings. It was defined through research by Dr. Ritchie Shoemaker and involves dysregulated innate immune activation, abnormal cytokine signaling, and a range of downstream effects on multiple organ systems. Genetic susceptibility, particularly involving HLA-DR variants, plays a documented role in determining who develops CIRS following exposure.
The condition is not uniformly recognized across mainstream medicine, but it has a growing body of peer-reviewed research and a substantial patient community. What makes nutrition questions especially difficult in CIRS is the heterogeneity of the condition itself. Patients present with vastly different symptom profiles, different degrees of immune dysregulation, different hormonal disruptions including MSH, VIP, and leptin pathway abnormalities, and different metabolic states. A nutritional approach that might be beneficial for one patient could be poorly tolerated by another.
Any discussion of intermittent fasting and CIRS must begin with this acknowledgment: the two bodies of literature have not been formally brought together. What follows is an examination of what each field tells us, and what the relevant intersection points might be, with careful honesty about where that reasoning is speculative.
What intermittent fasting research actually shows
Intermittent fasting is an umbrella term for various eating patterns that cycle between periods of eating and voluntary fasting. The most studied forms include time-restricted eating, typically eating within a 6 to 10 hour daily window, and alternate-day approaches. Research on intermittent fasting has grown substantially over the past decade, and several documented mechanisms are potentially relevant to inflammatory conditions.
Fasting periods have been shown to stimulate autophagy, the cellular process by which cells break down and recycle damaged components. A 2024 review in Cell Metabolism summarized research indicating that autophagy is suppressed during continuous fed states and upregulated during fasting periods, with potential implications for cellular housekeeping functions. Autophagy has been proposed as relevant to immune regulation, though its role in human inflammatory diseases is still being characterized.
Intermittent fasting has also been associated with reductions in circulating inflammatory markers in multiple studies. A 2024 meta-analysis in Obesity Reviews examining randomized controlled trials of intermittent fasting found significant reductions in C-reactive protein and interleukin-6 in overweight and obese populations. Importantly, most of this research was conducted in metabolically healthy or overweight populations, not in people with systemic inflammatory conditions driven by biotoxin exposure. The mechanism of inflammation in CIRS involves innate immune dysregulation that differs from the metabolic inflammation studied in most intermittent fasting research.
Fasting has also been investigated for its effects on the gut microbiome, with some studies suggesting it may promote microbial diversity and reduce intestinal permeability. Gut dysfunction is common in CIRS, and some clinicians working in this space consider gut support an important component of management. However, whether fasting-induced microbiome changes would be beneficial or neutral in CIRS-specific gut dysfunction is not known.
The potential concerns with fasting in CIRS
Several features of CIRS biology raise genuine caution about intermittent fasting, and they deserve equal weight with the potential benefits.
CIRS patients frequently have disrupted leptin signaling. Leptin, a hormone produced by fat cells, plays roles in energy regulation, immune function, and appetite control. Research by Dr. Shoemaker and colleagues has documented that elevated leptin and leptin resistance are common findings in CIRS patients, contributing to fatigue and immune dysregulation. Fasting affects leptin levels, and the implications of manipulating leptin dynamics in a system where leptin regulation is already abnormal are not well understood.
Many CIRS patients already experience significant fatigue, cognitive impairment, and difficulty maintaining stable energy. The adaptation period for intermittent fasting, which can involve several weeks of increased fatigue and brain fog as the body adjusts to metabolic flexibility, may be poorly tolerated by patients who are already operating at minimal functional reserve. What is a temporary adaptation cost for a healthy person could represent a significant setback for someone with CIRS.
Adrenal function is also relevant. Some CIRS patients have dysregulated cortisol patterns. Fasting is a physiological stressor that activates the hypothalamic-pituitary-adrenal axis and raises cortisol. In a patient whose HPA axis regulation is already compromised, this additional stressor may not be well-tolerated.
There is also the question of detoxification. Some CIRS treatment protocols include dietary components specifically to support biotoxin clearance, such as adequate fiber for bile acid binding. Fasting regimens that significantly restrict eating windows may complicate the implementation of these dietary components in the ways and amounts recommended by treating clinicians.
What the evidence gap means in practice
The absence of direct CIRS-specific research on intermittent fasting is not a reason to assume it's safe, and it's not a reason to assume it's harmful. It means there is no clinical basis for a recommendation in either direction. Extrapolating from general population intermittent fasting research to CIRS patients involves significant uncertainty because the underlying biology is different.
Some functional medicine practitioners working with CIRS patients have incorporated time-restricted eating into comprehensive treatment protocols, reporting anecdotal tolerability. Others report that patients with significant fatigue and metabolic disruption do better with regular, structured eating patterns that maintain stable glucose and support medication and supplement timing. No rigorous comparison of these approaches in CIRS patients exists in the published literature as of 2025.
The role of environment alongside any dietary approach
Whatever nutritional approach a CIRS patient pursues in consultation with their clinician, environmental control remains foundational. The Shoemaker protocol is explicit that removal from ongoing biotoxin exposure is the prerequisite for recovery. No dietary intervention, including intermittent fasting, operates effectively if the source exposure is ongoing.
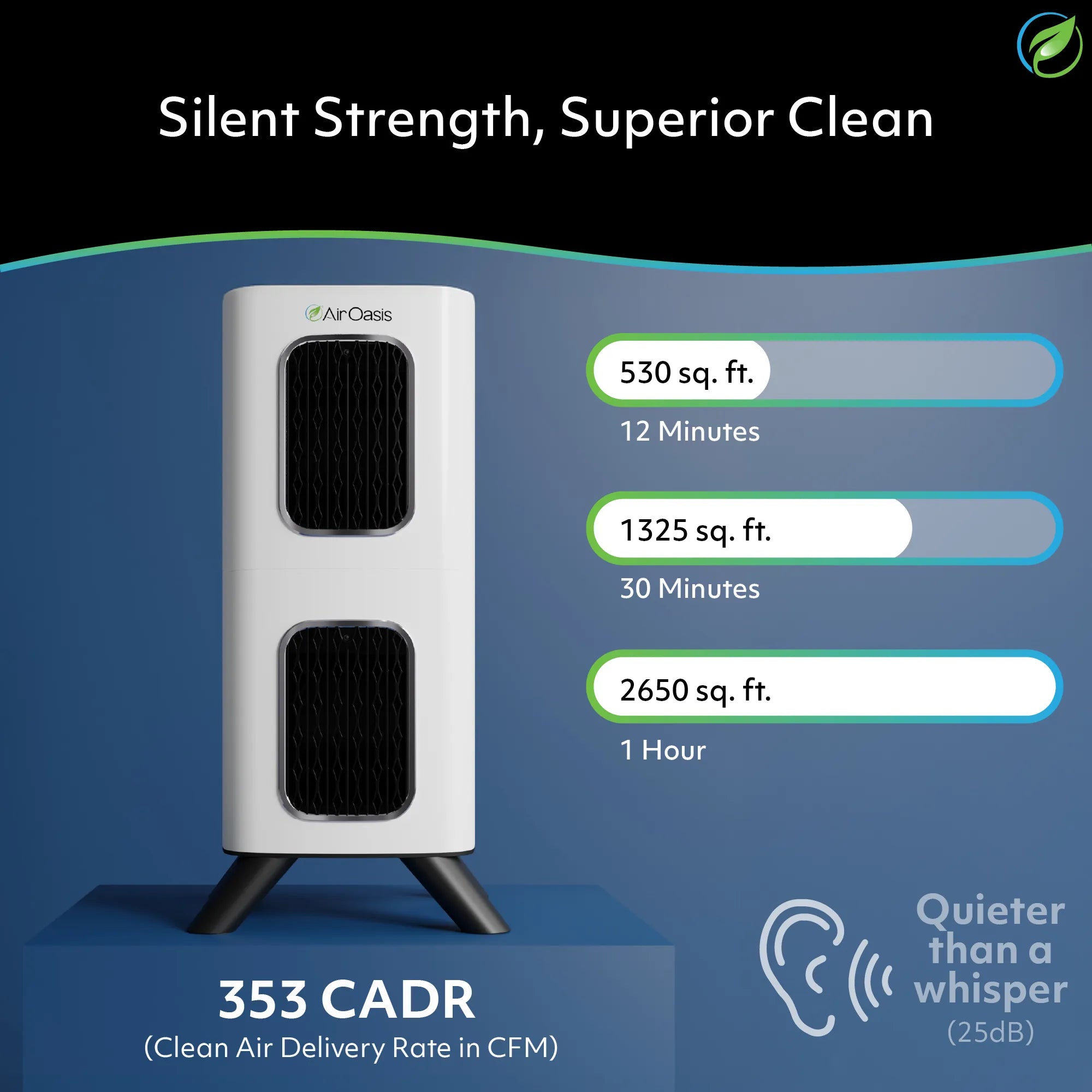
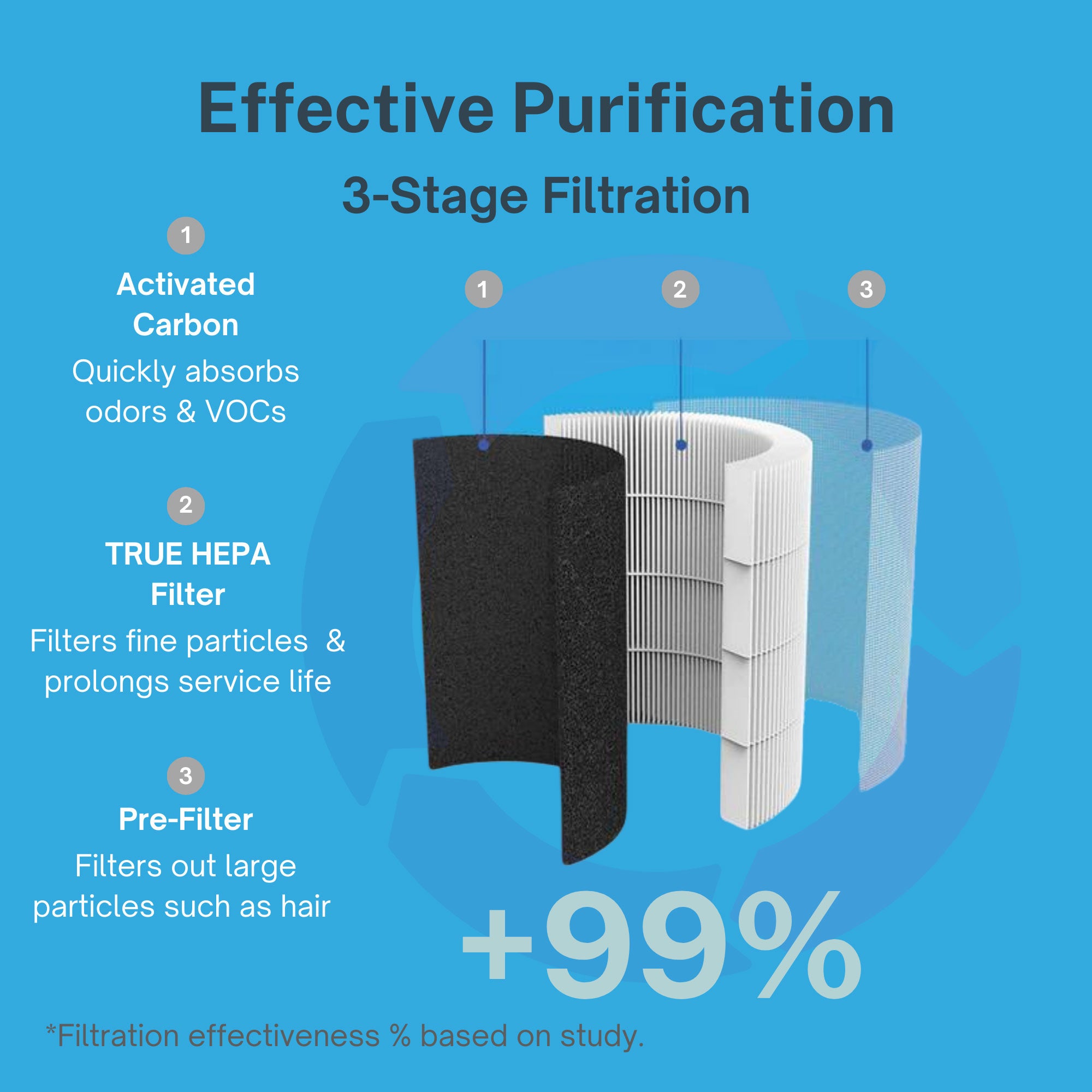
Reducing airborne biotoxin burden in the home is where air purification plays a direct, practical role. The iAdaptAir by Air Oasis uses true HEPA filtration to capture airborne mold spores, activated carbon to address mycotoxin-related volatile organic compounds, and UV-C light and bipolar ionization to address airborne biological contaminants. It's CARB-certified ozone-free, critical for CIRS patients who often have concurrent chemical sensitivities, and includes a removable WiFi module for those managing electromagnetic sensitivities. For CIRS recovery, reducing the ongoing environmental load is not optional. It is the foundation on which every other therapeutic effort rests.
Consult your clinician before experimenting
If you're managing CIRS and considering intermittent fasting, the right starting point is a conversation with a clinician experienced in CIRS treatment, not a wellness blog or a community forum. Your leptin levels, your fatigue severity, your adrenal function, your current treatment stage, and your ability to maintain the dietary components of your protocol all matter to whether fasting might be appropriate for you, contraindicated, or simply premature given where you are in treatment.
This is a question the research hasn't answered yet. That's an honest place to start. Shop the iAdaptAir at Air Oasis and make your indoor environment as clean as it can be while the science catches up. Breathe Better, Live Better.